Since “marriage for all” became possible in Germany, rainbow families have been largely placed on an equal footing with heterosexual married couples in many areas. However, on the path to having a child, there are still a number of hurdles to overcome, ranging from the (medical) realization of parenthood to the legal recognition of parenthood and complex adoption procedures. In addition, there are differing regulations in the legislation of the federal states, in the guidelines applicable to treating physicians issued by the responsible medical associations, and in the financial support provided by potential cost bearers.
As your consulting physicians, we competently support you with the medical aspects of your journey towards having a child. As we are not permitted to provide legal advice, you will find below a selection of links that address relevant issues and questions from a legal perspective in detail.
The team at the MVZ Pan Institute specializes in the interdisciplinary care of couples with an unfulfilled desire to have children. Lesbian couples (cisgender female couples) are also optimally supported on their journey towards starting their own family.
Assisted reproduction treatment methods:
In addition to the options of becoming a foster family or adopting a child, assisted reproduction is a good option for lesbian couples on their path to parenthood.
Two different procedures using donor sperm from a sperm bank are available for assisted reproduction:
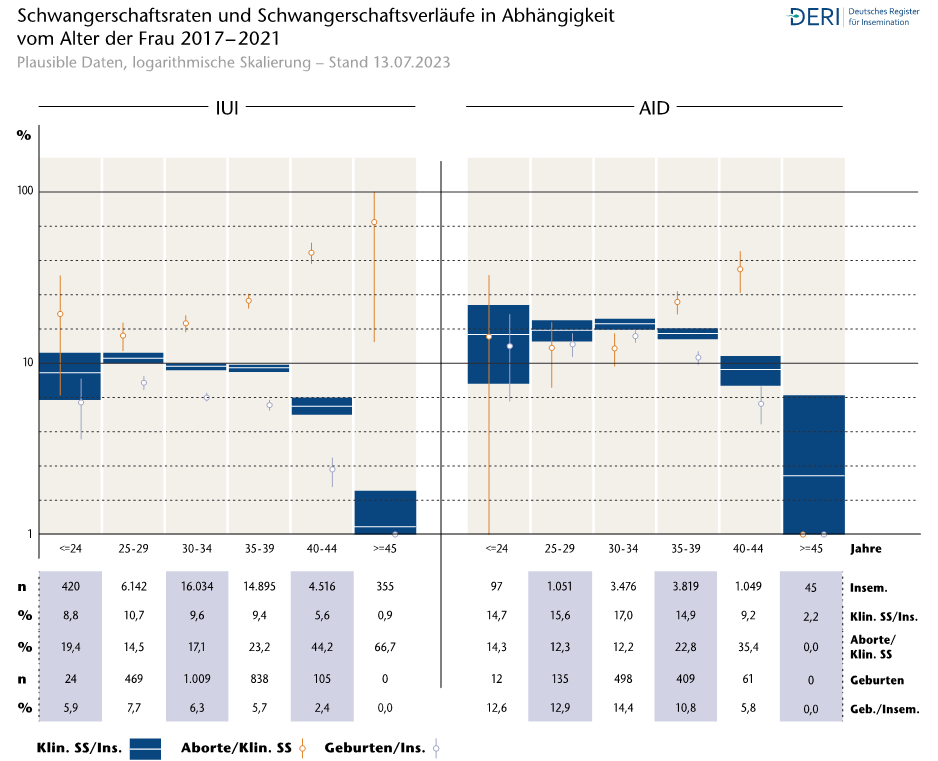
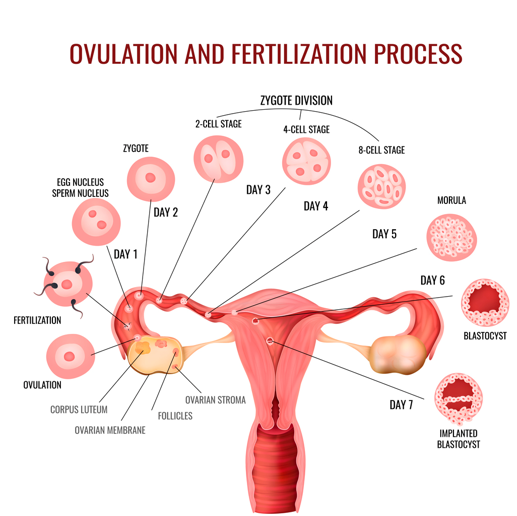
In intrauterine insemination, donor sperm is introduced directly into the uterine cavity using a thin catheter. Fertilization of the egg then occurs naturally.
In cases of cycle disorders, accompanying hormonal stimulation may be carried out.
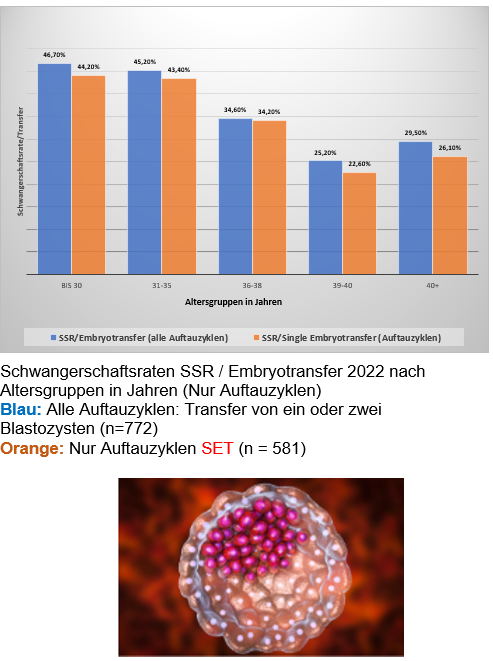
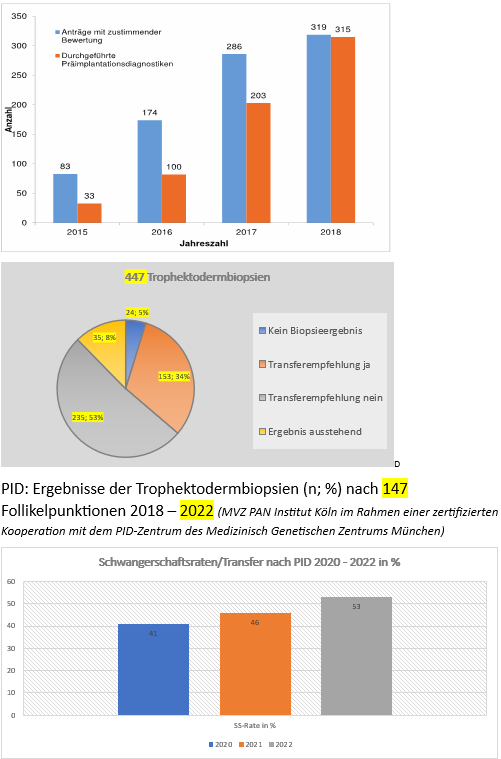
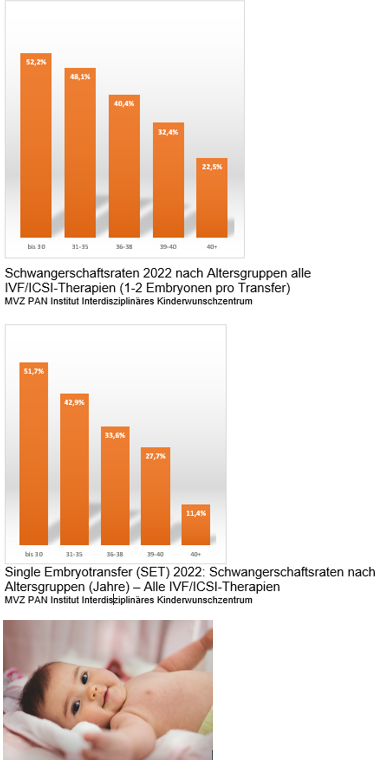
If treatments using intrauterine insemination are repeatedly unsuccessful or if the chances of success of insemination therapy are assessed as too low from the outset, assisted reproduction using IVF or ICSI may also be considered. In this process, the egg cell is fertilized with the sperm cell artificially in the laboratory, and the fertilized egg(s), now embryo(s), are then transferred to the uterus.
As part of a consultation, both treatment methods are explained in detail, including the procedure, chances of success, risks and side effects, costs, and the basic bureaucratic requirements.
We would like to inform you in advance about the necessary prerequisites for treatment at our fertility center:
You must already be married before starting fertility treatment. In addition, prior to the start of fertility therapy, notarized family law counseling is required, and we also recommend psychological counseling regarding the medical, emotional, and social aspects and challenges of heterologous fertility treatment (i.e. using donor sperm).
In counseling, diagnostics, and therapy, we are guided by your individual situation, wishes, and needs, based on national and international medical guidelines and recommendations. What unites us is the shared goal of helping you fulfill your desire to have a child as soon as possible.
The costs of fertility treatment through assisted reproduction are usually not covered by health insurance companies and must be borne by the couples themselves. Other subsidies (e.g. from the state of North Rhine-Westphalia) are generally not granted.
For assisted reproduction as part of fertility treatment for lesbian couples, donor sperm from a certified sperm bank is used. Sperm donors must meet strict health requirements (see also the German Sperm Donor Register Act: https://www.gesetze-im-internet.de/saregg/BJNR251310017.html). Prior to donation, donors undergo comprehensive medical examinations and a thorough medical history assessment with regard to chronic and genetic diseases. Transmissible diseases are also excluded.
We cooperate with the following institutions (for foreign sperm banks, only specific, designated donors may be used/ordered in Germany):
Erlangen Sperm Bank
European Sperm Bank
Cryos Denmark
As part of an initial consultation, all questions are clarified and patients are informed in detail about the individual steps of diagnostics and treatment as well as the applicable legal and organizational framework. Once the medical aspects of the procedure have been clarified, contact can be made with the sperm bank to select a suitable sperm donor, and the required notarized and psychological counseling can take place.
If you are a cisgender, married female couple wishing to realize your desire to have a child through intrauterine insemination or IVF/ICSI (“in vitro fertilization”) treatment using donor sperm, please feel free to contact us.
We look forward to meeting you!
FURTHER READING (from the NRW Family Portal):
The Rainbow Portal is an information service provided by the Federal Ministry for Family Affairs, Senior Citizens, Women and Youth. Details on adoption law and further legal framework conditions for rainbow families can be found here: www.regenbogenportal.de
In addition, the Ministry for Family Affairs of the State of North Rhine-Westphalia provides information on this topic: www.mkjfgfi.nrw/lsbtiq
Further information on the topic “Experiencing family diversity in early childhood education” can be found on the NRW daycare portal: www.kita.nrw.de
Comprehensive information on family formation by same-sex couples can be found on the website of the German Lesbian and Gay Association: www.lsvd.de
The “Rainbow Family Counseling Competence” portal of the German Lesbian and Gay Association offers professionals in family-related counseling fields thematic lectures and day workshops on living with and counseling rainbow families: www.regenbogenkompetenz.de
rubicon e. V. provides counseling, health promotion, and support for lesbian, gay, bisexual, trans*, inter*, and queer individuals and groups: www.rubicon-koeln.de